
What current research actually shows about aging, muscle, hormones, sleep, stress, insulin resistance, and the myths that dominate the phrase slow metabolism.
By the Repeat Editorial Team Medically informed, evidence-based
| TL;DR THE 60-SECOND VERSION |
| • Metabolism does not crash at 30. A landmark 2021 study measuring more than 6,600 people found total daily energy expenditure, adjusted for body size, stays essentially flat from age 20 to 60, and only begins declining, by about 0.7% a year, after 60. |
| • What actually changes in your 30s and 40s is usually muscle mass and activity level, not some internal metabolic switch. Muscle is lost at roughly 3 to 8% per decade after 30 if untrained, and muscle tissue burns more at rest than fat tissue. |
| • A study of Hadza hunter-gatherers, among the most physically active people on Earth, found their total daily energy expenditure was statistically indistinguishable from sedentary Westerners, once adjusted for body size, a finding that reshaped how scientists think about exercise and calorie burn. |
| • Chronic stress, poor sleep, and hormonal shifts (thyroid, cortisol, insulin, and, for women, estrogen and progesterone) all influence metabolic rate and fat storage more than age itself does. |
| • “Starvation mode” from skipping a meal is a myth. Measurable metabolic slowdown from undereating generally requires 60 or more hours of near-total fasting, not one missed lunch. |
| • Metabolic flexibility, the ability to switch efficiently between burning fat and burning carbohydrate, is a defining feature of a healthy metabolism, and its breakdown is now considered central to insulin resistance. |
| • Two people at an identical body weight can have very different metabolic health depending on where their fat is stored. Visceral fat around the organs is far more metabolically damaging than subcutaneous fat under the skin, and a meaningful share of normal-weight people carry dangerous amounts of it. |
Metabolism is one of the most talked-about and least accurately understood concepts in health. It gets blamed for weight gain, credited for weight loss, and marketed as something that can be boosted with a tea, a supplement, or a morning routine. Very little of that popular picture matches what metabolic research actually shows. Metabolism is not a dial that quietly turns down the moment you turn 30, and it is not something a product can meaningfully speed up.
This article works through what is actually known about metabolic rate across the lifespan: why it changes with age, how muscle, hormones, sleep, and stress shape it, what metabolic flexibility and insulin resistance really mean, and why body weight alone is a surprisingly poor proxy for metabolic health. It also looks at a genuinely fascinating natural experiment, one of the most physically active populations on the planet, and at the specific myths about slow metabolism that marketing keeps recycling.
1. What Actually Happens to Metabolism After 30
The idea that metabolism begins a steady decline the moment you turn 30 is one of the most repeated claims in health media, and it does not hold up against the best available data. A landmark 2021 study in Science, led by anthropologist Herman Pontzer, measured total daily energy expenditure using doubly labeled water, the gold-standard method, in more than 6,600 people ranging from eight days old to 95 years old across 29 countries. After adjusting for body size and composition, the researchers found that energy expenditure remains essentially stable through the entire span from age 20 to 60, including during pregnancy, according to a summary from Duke Today.
Metabolic rate does eventually decline, just decades later than most people assume, and far more gradually. The same research found the slowdown does not begin until after age 60, and even then it proceeds at only about 0.7% per year. “Perhaps you’ve been told that it’s all downhill after 30 when it comes to your weight,” Pontzer noted, but the data suggest a changing metabolism is not actually the explanation for the weight gain many people experience during those middle decades.
So why does weight tend to creep up in the 30s and 40s anyway?
If total energy expenditure is not dropping, the thickening waistlines common in this age range have to come from somewhere else, and the research points to a combination of factors that have nothing to do with a slowing metabolic engine: gradually declining physical activity as work and family responsibilities increase, loss of muscle mass from reduced training, portion sizes and eating patterns that shift with lifestyle, and, in many cases, simply more years of a small but consistent calorie surplus compounding over time. None of these are about metabolism breaking down; they are about behavior and body composition changing while metabolic capacity itself stays largely intact.
2. Muscle Mass: The Biggest Lever You Actually Control
If age itself is not the main driver of metabolic change, muscle mass is one of the few levers that genuinely is. Muscle tissue is metabolically active at rest in a way that fat tissue is not, which means the composition of a person’s body, not simply their weight, has a direct effect on how many calories they burn while doing nothing at all. Without resistance training, adults lose roughly 3 to 8% of muscle mass per decade after age 30, a process called sarcopenia, with the rate of loss accelerating further after age 60, according to a review in PMC.
This is not a cosmetic issue. A 2019 review in the Journal of Obesity describes how sarcopenia reduces resting energy expenditure, everyday non-exercise movement, and locomotion economy simultaneously, creating conditions that favor fat gain even without any change in diet. The relationship also runs in both directions: reduced metabolic health and increased obesity independently accelerate muscle loss, which is part of why the two problems tend to compound each other over time rather than developing in isolation.
The encouraging half of this picture is that sarcopenia is not a fixed sentence. Resistance training reliably rebuilds muscle mass and strength at essentially any age, including in frail adults in their 80s and 90s, and the metabolic benefit shows up quickly: even a few weeks of progressive strength training can measurably improve markers of metabolic health independent of any change in body weight.
3. Signs Your Metabolism Isn’t Working Optimally
Because true metabolic rate is hard to feel directly, most of the signals worth paying attention to are really signals of metabolic flexibility and insulin sensitivity breaking down, not the total number of calories being burned. The table below distinguishes vague, commonly cited symptoms from the specific, measurable markers that clinicians actually use to assess metabolic health.
Table 1. Common self-reported signs versus the clinical markers that actually confirm metabolic dysfunction.
| Commonly reported sign | What it may reflect | How it is actually confirmed |
|---|---|---|
| Energy crashes after carbohydrate-heavy meals | Impaired glucose clearance, reduced insulin sensitivity | Fasting glucose, HbA1c, oral glucose tolerance test |
| Difficulty losing fat despite consistent effort | Reduced NEAT, muscle loss, or an underestimated intake | DEXA scan, tracked intake, resting metabolic rate testing |
| Persistent fatigue, cold intolerance, hair thinning | Possible thyroid dysfunction | TSH, free T4, free T3 blood panel |
| Increased abdominal fat at a stable body weight | Fat redistribution toward visceral storage | Waist circumference, waist-to-hip ratio, DEXA or CT imaging |
| Poor recovery from exercise, elevated resting heart rate | Chronic stress or inadequate sleep affecting the HPA axis | HRV tracking, sleep studies, cortisol rhythm testing where indicated |
None of the left-hand column items are diagnostic on their own, and it is worth resisting the temptation to self-diagnose a metabolic condition from symptoms alone. They are, however, a reasonable prompt to check the actual markers in the right-hand column with a clinician rather than reaching for a supplement marketed to fix a slow metabolism.
4. The Hormone Connection: Thyroid, Cortisol, Insulin, and Sex Hormones
Metabolic rate is under direct hormonal control, and disruption in any of several systems can meaningfully change how the body stores and burns energy, independent of diet or exercise habits.
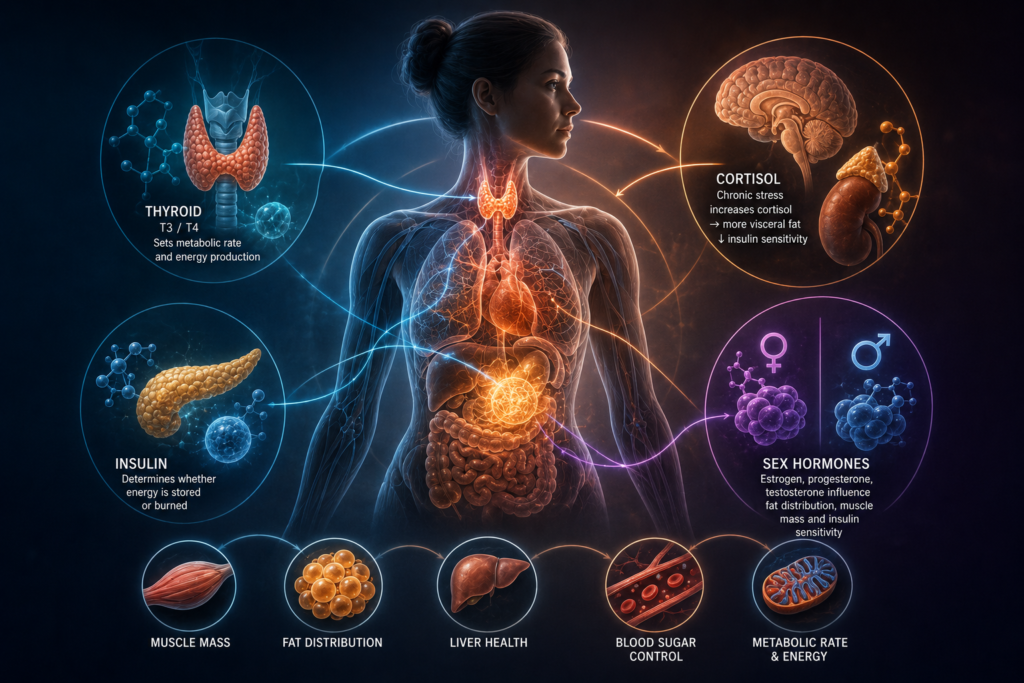
Thyroid
The thyroid gland sets the baseline pace of metabolism through the hormones T3 and T4. An underactive thyroid, hypothyroidism, is a genuine, well-documented medical cause of reduced metabolic rate, fatigue, weight gain, and cold intolerance, and it is diagnosed through a simple blood panel rather than guessed at from symptoms alone. It is also far less common than the volume of online content about it would suggest; most people experiencing a slow metabolism do not have a thyroid disorder, but for the minority who do, thyroid hormone replacement is a well-established and effective treatment.
Cortisol and chronic stress
Chronically elevated cortisol, covered in depth in Repeat’s article on women’s hormones, promotes fat storage specifically in the visceral, abdominal region and can worsen insulin sensitivity over time. This is a real, mechanistically understood pathway, distinct from the unsupported concept of adrenal fatigue.
Insulin
Insulin is arguably the single most important hormone for metabolic health, governing whether the body stores incoming fuel or burns it. Persistently elevated insulin, driven by insulin resistance, is covered in detail in Section 7.
Sex hormones
Estrogen, progesterone, and testosterone all directly influence fat distribution and insulin sensitivity. The decline in estrogen during perimenopause, for instance, is associated with a measurable shift toward abdominal fat storage and reduced insulin sensitivity, a pattern detailed in Repeat’s article on women’s hormones. Declining testosterone in aging men is similarly associated with reduced muscle mass and increased fat storage, reinforcing why hormonal health and metabolic health cannot be fully separated from one another.
5. Sleep and Metabolic Health
Few single interventions affect metabolic markers as quickly and as measurably as sleep. In a controlled study published in Diabetes, healthy men restricted to short sleep for just one week showed a measurable reduction in insulin sensitivity, confirming and extending earlier work from Karine Spiegel and Eve Van Cauter’s laboratory, which found that even a few nights of sleep debt produced glucose tolerance impairments comparable to what is seen in early-stage prediabetes.
Sleep loss disrupts metabolic health through several overlapping pathways: it raises evening cortisol, decreases the satiety hormone leptin while increasing the hunger hormone ghrelin, and directly reduces insulin sensitivity independent of any change in diet. The practical implication is that sleep is not a passive backdrop to metabolic health, it is one of the more directly modifiable levers available, arguably on par with diet and exercise for its speed of effect on insulin sensitivity specifically.
6. Chronic Stress and Metabolism
Chronic, unresolved stress affects metabolism through the same HPA axis pathway discussed in Repeat’s cortisol coverage: sustained cortisol elevation promotes preferential fat storage in the visceral depot, raises blood glucose, and, over time, contributes to insulin resistance. Stress also indirectly undermines metabolic health by disrupting sleep and often shifting food choices toward the highly palatable, energy-dense foods that are easiest to over-consume.
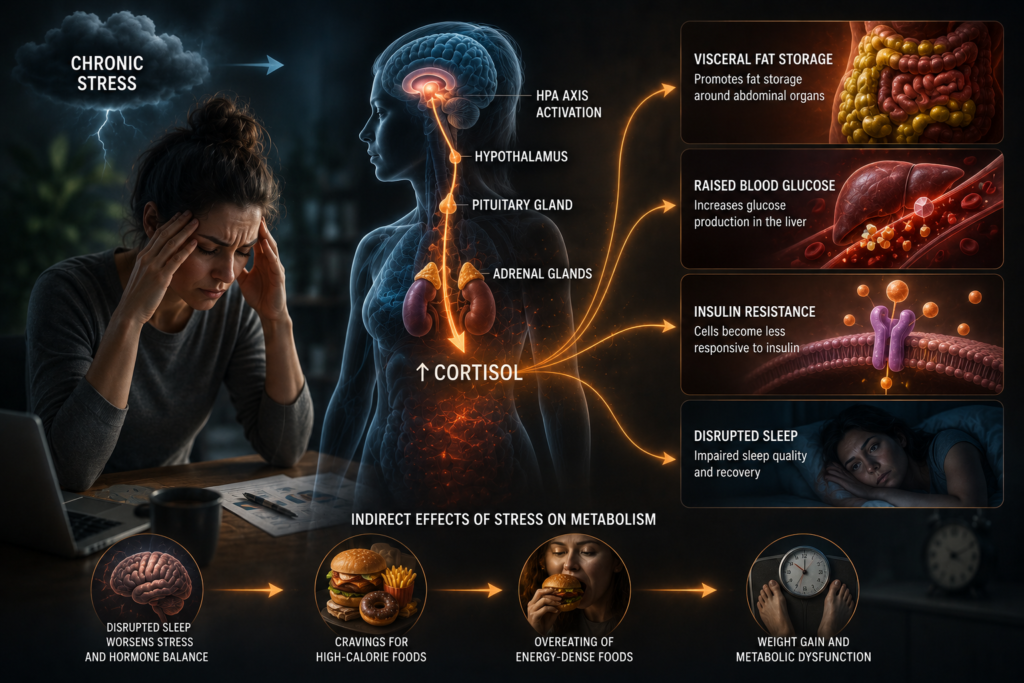
This does not mean stress alone causes weight gain in every case, metabolic outcomes are always multifactorial, but chronic stress is a legitimate, evidence-backed contributor to metabolic dysfunction rather than a vague wellness talking point, which is why stress management belongs in the same practical category as diet, exercise, and sleep rather than being treated as optional.
7. Insulin Resistance and Metabolic Flexibility
Metabolic flexibility is the capacity of the body to switch efficiently between burning fat and burning carbohydrate depending on what fuel is available, a concept formally defined by researcher David Kelley in 1999 after observing that lean individuals adapted fuel use smoothly around fasting and meals, while insulin-resistant individuals did not, according to a review in Endocrine Reviews.
The connection to insulin resistance is direct rather than incidental. The same review states plainly that metabolic inflexibility is at the core of the pathophysiology of insulin resistance. In a metabolically healthy person, muscle tissue readily shifts toward burning fat during fasting and toward burning glucose after a meal, guided by insulin. In insulin resistance, this switching mechanism breaks down: muscle cells remain less able to take up and oxidize fat efficiently, fat begins accumulating inside muscle tissue itself, and the body increasingly defaults to burning glucose regardless of what is actually needed, which in turn worsens blood sugar control and drives further fat storage.
Practically, the interventions that improve metabolic flexibility overlap heavily with the interventions that improve insulin sensitivity more broadly: regular exercise, particularly a mix of aerobic and resistance training, adequate sleep, and reduced intake of ultra-processed, rapidly digested carbohydrates eaten in excess of what the body can use. Metabolic flexibility is not something a supplement restores; it responds specifically to the same handful of lifestyle inputs that show up throughout this article.
8. Ancient Wisdom, Modern Proof: What Hunter-Gatherers Reveal About Human Metabolism
One of the more genuinely surprising findings in modern metabolic science did not come from a lab in a wealthy country. It came from measuring the Hadza, a population of traditional hunter-gatherers in northern Tanzania whose daily life involves walking long distances to forage for wild plants and hunt game. Researcher Herman Pontzer and colleagues used doubly labeled water to directly measure the Hadza’s total daily energy expenditure for the first time in a foraging population, publishing the results in PLOS One.
The result overturned a widely held assumption. Despite Hadza physical activity levels being substantially higher than those of Westerners, their total daily energy expenditure, after adjusting for body size, was statistically indistinguishable from that of sedentary adults in the United States and Europe, as reported by ScienceDaily. “These results highlight the complexity of energy expenditure,” Pontzer said at the time. “It’s not simply a function of physical activity. Our metabolic rates may be more a reflection of our shared evolutionary past than our diverse modern lifestyles.”
The constrained energy expenditure model
This finding, and similar results in athletes and other physically demanding populations, led Pontzer to propose what is now called the constrained energy expenditure model: rather than total calorie burn simply adding up linearly as activity increases, the body appears to actively regulate total energy expenditure within a relatively narrow range, dialing down energy allocated to other processes, such as inflammation, reproduction, and stress hormone production, when physical activity rises substantially. The Hadza were not burning more calories overall than sedentary Westerners; their bodies appeared to be reallocating a similar total energy budget toward movement instead.
It is worth noting this interpretation has been contested. Some researchers, in a response published by Active Living Research, have argued the comparison should have been made per kilogram of body weight rather than using total expenditure, given that the Hadza in the study were substantially leaner than the Western comparison group, which would produce a different conclusion about the relationship between activity and body weight. The debate itself is a useful reminder that even well-designed studies on metabolism deserve scrutiny rather than being converted directly into simple headlines.
What is not in dispute is the practical takeaway the researchers themselves emphasized: even if exercise contributes less to total daily calorie burn than commonly assumed, physical activity remains essential for health for reasons entirely separate from calorie accounting, including the muscle mass, cardiovascular fitness, and insulin sensitivity benefits covered throughout this article. The Hadza data complicates the simple story that exercise is primarily a calorie-burning tool; it does not undermine the case for exercise itself.
9. Marketing vs. Medicine: Common Myths About Slow Metabolism
The starvation mode myth
Few metabolism myths are as persistent as the idea that skipping a single meal, or eating too little for a day, triggers starvation mode and permanently slows metabolic rate. The evidence does not support this at the timescales most people worry about. Reviews of the fasting physiology literature note that measurable reductions in resting metabolic rate generally do not begin until roughly 60 hours of near-total fasting, with some studies finding no effect until 72 to 96 hours, and even then the decline is modest, on the order of a single-digit percentage, according to a review of the fasting research summarized on Leangains. Genuine, sustained metabolic adaptation to underfeeding is real at the extremes, sustained intake below roughly half of caloric needs for weeks or months can produce a measurable slowdown, but that describes prolonged, severe caloric restriction, not an occasional missed lunch or a single day of lighter eating.
Metabolism-boosting foods and supplements
No food, tea, or supplement produces a meaningful, sustained increase in metabolic rate. A clinical overview from Gundersen Health System states directly that there is no evidence supporting the use of supplements to boost metabolism, noting that compounds like green tea extract and capsaicin from spicy peppers have shown a measurable thermogenic effect in some studies, but one small enough to be practically insignificant. Muscle mass, not any ingestible product, remains the only durable lever for raising resting metabolic rate covered anywhere in the current research.
Wearables and at-home metabolic testing
A newer category of marketing claim involves consumer devices and at-home tests promising a precise metabolic rate or metabolic age reading. Bioelectrical impedance devices, in particular, correlate only moderately with gold-standard measurements like DEXA or doubly labeled water; the same limitation discussed for visceral fat estimation in Section 11 applies broadly here. These tools can be useful for tracking a personal trend over time if used consistently, but a single reading should be treated as a rough estimate rather than a clinical-grade diagnosis.
Table 2. Popular metabolism claims ranked by how strong the current evidence actually is.
| Claim | Evidence status | What is actually known |
|---|---|---|
| Resistance training raises resting metabolic rate | Strong | Direct mechanistic link via increased muscle mass; well replicated |
| Metabolism is essentially stable from 20 to 60 | Strong | Confirmed by large-scale doubly labeled water measurement across 29 countries |
| Sleep restriction reduces insulin sensitivity | Strong | Repeatedly demonstrated in controlled laboratory studies since the late 1990s |
| Skipping one meal triggers starvation mode | Not supported | Measurable slowdown requires 60+ hours of near-total fasting |
| Metabolism-boosting teas and supplements | Not supported | No clinically meaningful effect on resting metabolic rate demonstrated |
| Consumer bioelectrical impedance devices | Preliminary, moderate accuracy | Useful for personal trends; not a substitute for DEXA or clinical testing |
10. How to Actually Support Your Metabolism: Exercise and Nutrition
Exercise
- Resistance training two to three times a week is the single most direct lever for preserving and building the muscle mass that drives resting metabolic rate.
- Cardiorespiratory fitness, built through a mix of Zone 2 and higher-intensity work, supports metabolic flexibility and insulin sensitivity independent of muscle mass.
- Non-exercise activity, walking, standing, general daily movement, adds up meaningfully over a week and is often the first thing that quietly declines in busy decades, contributing more to the weight changes described in Section 1 than most people assume.
Nutrition
- Adequate protein intake supports both muscle maintenance and the thermic effect of food, since protein requires more energy to digest than fat or carbohydrate.
- Fiber and whole-food carbohydrate sources support the short-chain fatty acid production and glycemic stability that underpin metabolic flexibility, a topic covered in depth in Repeat’s gut health article.
- Minimizing ultra-processed, rapidly absorbed carbohydrate in excess of activity level is one of the more consistently supported dietary levers for preserving insulin sensitivity over time.
- Consistent meal timing and adequate total intake, rather than chronic under-eating, better support the metabolic flexibility and hormonal stability described throughout this article.
11. Body Composition: Why the Number on the Scale Is the Wrong Metric
Body composition vs. body weight
Body weight tells you almost nothing about the ratio of muscle to fat, or where that fat is distributed, both of which matter far more for metabolic health than total mass alone. Two people at an identical weight and even an identical BMI can have dramatically different metabolic profiles depending on body composition, which is why clinicians increasingly favor direct composition measurement, DEXA scans being the most accessible gold standard, over weight or BMI alone when assessing metabolic risk.
Visceral fat: the metabolically active kind
Not all body fat behaves the same way. Subcutaneous fat, stored just beneath the skin, functions mostly as passive energy storage. Visceral fat, stored deeper around the abdominal organs, is metabolically active tissue that releases inflammatory signals directly into the bloodstream via the portal vein, according to a clinical overview from BodySpec. This direct route to the liver is part of why visceral fat is far more strongly associated with insulin resistance, elevated blood pressure, and cardiovascular disease risk than a comparable amount of subcutaneous fat.
Why two people at the same weight can have completely different metabolism
This distinction explains one of the more counterintuitive findings in body composition research: a meaningful share of people with a normal body weight and a normal-looking waistline are carrying disproportionate amounts of visceral fat internally, a phenotype researchers call TOFI, thin outside, fat inside. These individuals face an elevated risk of insulin resistance and type 2 diabetes despite appearing lean, and estimates place the prevalence of this metabolically obese, normal-weight pattern at roughly 13 to 18% of the population, according to a review in Nutrition Research Reviews. The reverse pattern exists too: some individuals classified as clinically obese by BMI carry proportionally less visceral fat and more subcutaneous fat, and show comparatively healthier metabolic markers than their BMI alone would predict.
The practical implication is direct: body weight and BMI are useful population-level screening tools, but neither is a reliable individual measure of metabolic health. Waist circumference is a far better free proxy for visceral fat than weight or BMI alone, and where available, direct imaging remains the most accurate way to know where fat is actually being stored, and therefore how much metabolic risk it actually represents.
Metabolism does not quietly collapse the moment you turn 30, and it is not something a tea, a supplement, or a wearable device can meaningfully fix. What the best current research actually shows is more specific and more useful: total energy expenditure stays remarkably stable through most of adulthood, muscle mass is the biggest lever most people actually control, and sleep, stress, and insulin sensitivity influence metabolic health on a timescale of days and weeks rather than years. The Hadza data is a useful reminder that human metabolism evolved to be remarkably stable across very different lifestyles, which is exactly why chasing a faster metabolism is the wrong goal. Building and preserving muscle, protecting sleep, managing chronic stress, and eating in a way that supports insulin sensitivity remain the small list of interventions the evidence actually supports, and none of them require believing your metabolism is broken to begin with.
Sources & Further Reading
- Science, Daily energy expenditure through the human life course (Pontzer et al., 2021)
- Duke Today, Metabolism changes with age, just not when you might think
- PMC, Muscle tissue changes with aging
- Journal of Obesity, Sarcopenia and its implications for metabolic health
- Endocrine Reviews, Metabolic flexibility as an adaptation to energy resources and requirements in health and disease
- Diabetes (American Diabetes Association), Sleep restriction for 1 week reduces insulin sensitivity in healthy men
- PLOS One, Hunter-gatherer energetics and human obesity (Pontzer et al., 2012)
- ScienceDaily, Hunter-gatherers, Westerners use same amount of energy, contrary to theory
- Active Living Research, Debunking the hunter-gatherer workout: ALR’s response
- Leangains, Top ten fasting myths debunked
- Gundersen Health System, 3 common myths about your metabolism
- BodySpec, Visceral fat vs. subcutaneous fat: understanding the differences
- Nutrition Research Reviews, Excess body fat in obese and normal-weight subjects
- Biology Insights, How to tell visceral fat vs subcutaneous fat
This article is for general informational purposes and does not constitute medical advice. Speak with a qualified healthcare provider, such as an endocrinologist or registered dietitian, before making significant changes to diet, exercise, fasting, or supplementation, particularly if you manage a metabolic or endocrine condition.

