
What the research actually shows about cortisol, PCOS, perimenopause, cycle-based training, and hormonal weight gain, and where the wellness industry gets ahead of the evidence.
By the Repeat Editorial Team Medically informed, evidence-based
| TL;DR THE 60-SECOND VERSION |
| • Cortisol is not the villain it is made out to be online. It is a normal, necessary stress hormone. What actually causes harm is chronic, unresolved stress that keeps the HPA axis switched on for too long, not cortisol itself. |
| • “Adrenal fatigue” is not a recognized medical diagnosis. Endocrinology bodies and systematic reviews have repeatedly found no evidence that adrenal glands can burn out from stress; the real, measurable phenomenon is HPA axis dysregulation. |
| • PCOS affects an estimated 10 to 13% of women of reproductive age worldwide, and up to 70% of those affected remain undiagnosed, according to the World Health Organization. It is a metabolic condition as much as a reproductive one. |
| • Perimenopause can last 7 to 10 years, and nearly 80% of women experience vasomotor symptoms such as hot flashes. New research on timing suggests starting hormone therapy earlier in the transition may carry long-term benefits, though it is not approved as a weight-loss treatment. |
| • One genuinely ancient, well-evidenced practice stands out: chasteberry (Vitex agnus-castus) has 2,500 years of documented use for menstrual complaints and now has real randomized trial data behind it. |
| • “Cycle syncing” your workouts and meals to match hormone phases is popular online, but current sports-science reviews find no consistent evidence that training or metabolism needs to change by cycle phase for most women. |
| • Menopausal weight gain is real and partly hormonal, driven by a shift toward abdominal fat storage as estrogen declines, but it is not fully explained by hormones alone, and terms like “estrogen dominance” are not recognized medical diagnoses. |
Women’s hormonal health has become one of the most heavily discussed, and most heavily marketed, corners of wellness content. Search almost any hormone by name and the results split cleanly into two categories: dense clinical literature written for specialists, and confident lifestyle content that borrows scientific language without much scientific rigor in between. The gap between those two worlds is where a lot of unnecessary anxiety, and a lot of unnecessary spending, tends to live.
This article works through five of the topics women ask about most: cortisol and the stress response, PCOS, perimenopause, whether training and eating really need to be synced to the menstrual cycle, and hormonal weight gain. Along the way, it also looks at where genuinely old, well-tested practices hold up under modern research, and where popular modern terms borrow the language of hormones without the evidence to match.
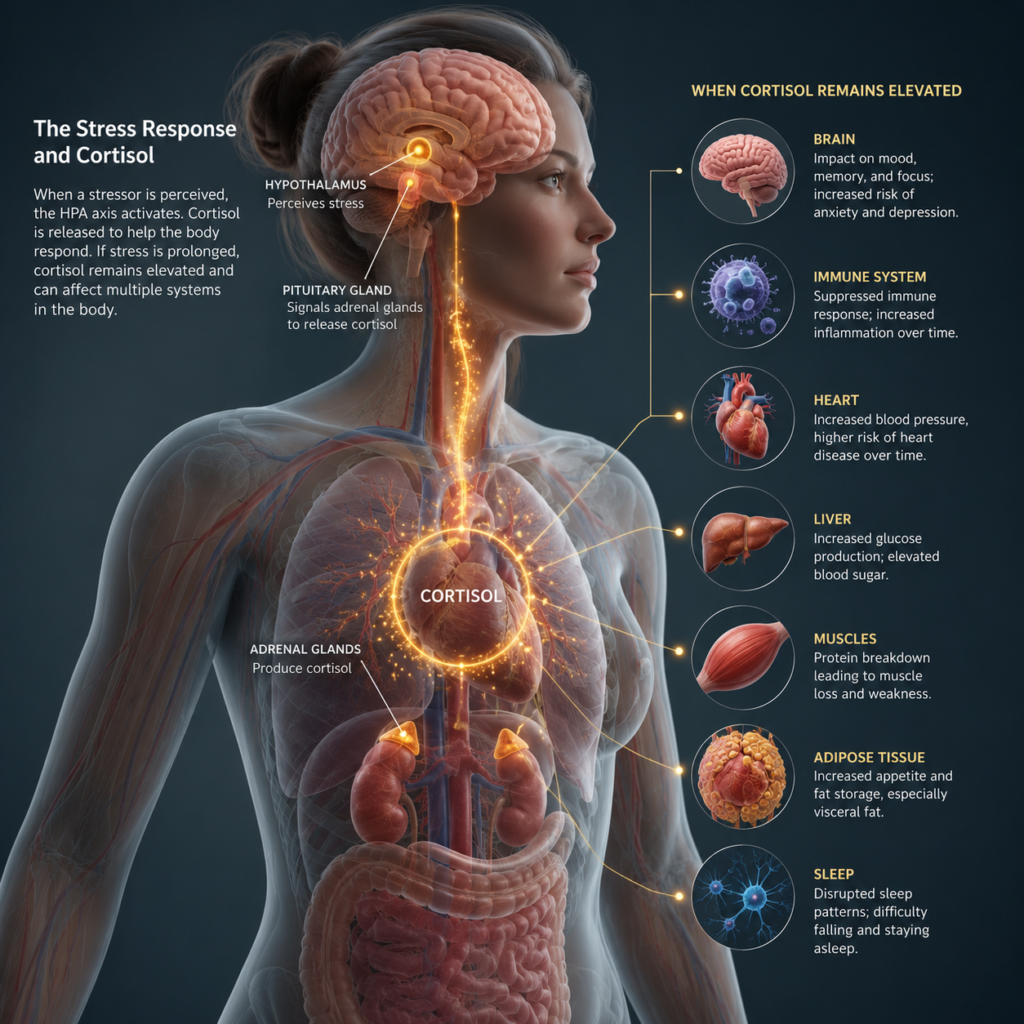
1. Cortisol: What It Actually Does, and What It Doesn’t
Cortisol has become shorthand online for almost everything that feels wrong: bloating, weight gain, poor sleep, irritability, a puffy face. In reality, cortisol is a normal, essential hormone produced by the adrenal glands as part of the hypothalamic-pituitary-adrenal axis, commonly called the HPA axis. It raises blood glucose for quick energy, temporarily suppresses non-urgent processes like digestion and immune activity, and sharpens alertness during a genuine stressor. Under normal conditions, once the stressor passes, cortisol feeds back negatively to the brain and the system quiets back down, according to a 2026 review of stress physiology.
What happens when the stress response never switches off
Problems arise not from cortisol itself but from the chronic activation of this system. When stress is repeated or unresolved, that negative feedback loop weakens and baseline cortisol output can drift upward over time. Research reviewed in Sterling Medical Center’s 2026 overview of HPA axis physiology links chronically elevated cortisol to documented effects including suppressed immune function, disrupted sleep architecture, increased visceral fat storage, impaired hippocampal function affecting memory and mood, and dysregulated inflammatory signaling. A 2025 review in the International Journal of Molecular Sciences goes further, describing how chronic HPA axis dysregulation shifts the balance of inflammatory cytokines in ways that are now considered a contributing mechanism in autoimmune conditions such as lupus and rheumatoid arthritis.
Adrenal fatigue: the diagnosis endocrinologists keep having to un-teach
This is where a real physiological phenomenon, HPA axis dysregulation, gets repackaged online as something else entirely: adrenal fatigue, the idea that chronically stressed adrenal glands eventually wear out and stop producing enough cortisol. It is a compelling story, and it is not supported by the evidence. A systematic review covering 58 studies, published in PMC, concluded there is no substantiation that adrenal fatigue is an actual medical condition, noting that salivary cortisol measured across a 24-hour period showed no meaningful difference between fatigued and healthy patients in the majority of the studies reviewed. The Endocrine Society does not recognize it as a legitimate diagnosis, and endocrinologists interviewed by TIME describe adrenal glands as functionally tireless: they may produce more cortisol under chronic stress, not less, and true adrenal failure is a separate, rare, and clinically distinct condition called Addison’s disease.
None of this means the symptoms attributed to adrenal fatigue are imaginary. Fatigue, brain fog, low mood, and salt or sugar cravings are real and common, and chronic stress plausibly contributes to many of them. What is misleading is the specific mechanism, and the industry of adrenal support supplements built on top of it. As one endocrinologist put it to Cedars-Sinai, stress can genuinely affect health without affecting the adrenal glands in the way the popular theory describes; the more clinically useful frame is HPA axis dysregulation, a real, measurable, and treatable pattern rather than a gland running out of fuel.
Table 1. Adrenal fatigue versus the recognized clinical conditions it is often confused with.
| Term | Medically recognized? | What is actually happening |
|---|---|---|
| Adrenal fatigue | No | Popular term for chronic stress symptoms; not supported by cortisol testing or systematic review evidence |
| HPA axis dysregulation | Yes | A measurable disruption in the cortisol rhythm and feedback loop under chronic stress |
| Addison’s disease | Yes (rare) | True adrenal insufficiency, usually autoimmune in origin, confirmed by ACTH stimulation testing |
| Cushing’s syndrome | Yes (rare) | True cortisol excess, often from a tumor or prolonged steroid medication use |
2. PCOS: The Most Common Hormonal Condition Few People Understand Well
Polycystic ovary syndrome is, by a wide margin, the most common hormonal disorder in women of reproductive age, affecting an estimated 10 to 13% of women globally, according to the World Health Organization. The same source estimates that up to 70% of affected women remain undiagnosed, often for years, because symptoms such as irregular periods, acne, or weight changes are easy to attribute to other causes.
How PCOS is actually diagnosed
PCOS is diagnosed using the Rotterdam criteria, which require at least two of three features: irregular or absent ovulation, clinical or biochemical signs of excess androgens such as persistent acne or hirsutism, and polycystic ovarian morphology visible on ultrasound. Contrary to what the name implies, having ovarian cysts alone does not mean a diagnosis of PCOS, and a diagnosis of PCOS does not require visible cysts at all. This is one of the more common points of confusion, since the name describes an ultrasound finding rather than the underlying hormonal condition.
Insulin resistance sits at the center of it
PCOS is as much a metabolic condition as a reproductive one. Insulin resistance is present in most women with PCOS regardless of body weight, and it worsens the hormonal picture directly: excess insulin stimulates the ovaries to produce more androgens, which in turn disrupts ovulation. This is why first-line treatment recommendations consistently include lifestyle interventions targeting insulin sensitivity rather than only hormone-focused medication.
What the supplement evidence actually says
Inositol supplements are widely marketed for PCOS, and the picture here is more nuanced than most product pages suggest. A systematic review and meta-analysis that directly informed the 2023 international evidence-based PCOS guidelines, published in the Journal of Clinical Endocrinology and Metabolism, concluded that the evidence supporting inositol for PCOS management is limited and inconclusive, while noting some benefit for specific metabolic measures. A separate 2026 umbrella review in Frontiers in Endocrinology assessed 85 evidence items across 13 meta-analyses and found no high-quality evidence at all; 41% of the evidence base was rated very low quality by GRADE criteria. This does not mean inositol is useless, myo-inositol in particular shows real signal for improving insulin sensitivity, but it does mean the confident marketing claims outrun what has actually been demonstrated with rigor.
Metformin remains the more established pharmacological option for the metabolic side of PCOS, and current guidelines position lifestyle change, including regular physical activity, dietary pattern, and sleep, as the first and best-supported intervention for most women, with medication added based on individual symptoms and goals.
3. Perimenopause: The Long Transition Few People Are Prepared For
Perimenopause is the transitional period leading up to menopause, marked by increasingly erratic hormone fluctuations while menstruation is still occurring. It is not brief. Vasomotor symptoms such as hot flashes affect an estimated 80% of women, with roughly half reporting daily symptoms that can persist for 7 to 10 years, according to a 2026 clinical review in American Family Physician. Sleep disturbance, mood changes, and genitourinary symptoms affect a further 45 to 80% of women, and together these symptoms can meaningfully affect quality of life, work, and relationships for the better part of a decade.
Timing may matter more than previously thought
Hormone therapy has had a genuinely turbulent history: use fell sharply after the Women’s Health Initiative raised cardiovascular and cancer concerns in the early 2000s, concerns that later analysis showed had been significantly overstated for most healthy women starting therapy near the onset of menopause. New research presented at The Menopause Society’s 2025 Annual Meeting adds a further layer: a large-scale analysis suggested that starting estrogen therapy during perimenopause itself, rather than waiting until after the final period, may carry additional long-term health benefits, a hypothesis researchers are calling the timing or window of opportunity effect. Data from Epic’s Cosmos health record dataset, covering more than 300 million patients, independently found hormone therapy prescriptions rose 86% between 2021 and late 2025, reflecting this shift in clinical thinking.
A note of caution belongs here too: hormone therapy is not recommended solely for preventing chronic disease, and it is explicitly not a weight-loss treatment, per the same American Family Physician review, though it is well supported for symptom relief and for preventing osteoporosis. Decisions about hormone therapy remain highly individual and depend on personal and family health history, which is exactly the kind of conversation worth having directly with a clinician rather than settling through a wellness influencer’s personal protocol.
4. Ancient Wisdom, Modern Proof: What Actually Holds Up
As with most areas of health, women’s hormonal wellness has its own long history of traditional practice, and some of it has aged considerably better than others under modern clinical study. Two examples are worth examining closely, because they land on opposite ends of the evidence spectrum despite both being framed as ancient wisdom today.
Chasteberry: 2,500 years of use, and now real trial data
Chasteberry, the fruit of the Vitex agnus-castus tree, has been used in women’s medicine for roughly 2,500 years, appearing in the writings of ancient Egyptian, Greek, and Roman physicians. Hippocrates himself used chasteberry preparations to stimulate milk production in new mothers and to treat menstrual complaints, according to a clinical review published by the American Academy of Family Physicians. Unlike most herbal remedies from antiquity, chasteberry did not fade into folklore. It was formally re-evaluated by European clinicians through the twentieth century, is listed in the German Commission E monographs for premenstrual complaints and cyclical breast tenderness, and has since accumulated real randomized controlled trial data.
A meta-analysis of double-blind, placebo-controlled trials published in Phytomedicine found that women taking standardized chasteberry extract were more than twice as likely to see meaningful symptom relief from PMS compared with placebo, a relative risk of 2.57. Mechanistically, chasteberry does not contain hormones or mimic estrogen; it appears to act on dopamine receptors in the pituitary gland, which indirectly helps normalize prolactin levels and support a more regular luteal phase. This is a rare case where a 2,500-year-old remedy and a modern meta-analysis are telling largely the same story.
Postpartum confinement: real cross-cultural wisdom, mixed modern evidence
Postpartum confinement, structured periods of rest, restricted activity, and family support following childbirth, appear independently in more than twenty countries across Asia, Africa, Europe, and the Americas, typically lasting 30 to 40 days, according to a historical overview on Grokipedia. The best-documented version is the Chinese practice of zuo yuezi, or doing the month. The honest picture from modern research is mixed rather than uniformly supportive: a systematic review in PLOS One found very little direct evidence that the specific restrictive practices, such as avoiding bathing or ventilation, improve recovery, though higher adherence was associated with lower postpartum depression scores and lower reported fatigue in several of the included studies, likely reflecting the concentrated family and social support that comes bundled with the tradition rather than the restrictions themselves.
The throughline across both examples is informative. Where a traditional practice has a plausible, testable mechanism, such as a specific plant compound acting on a specific receptor, modern trials have increasingly been able to confirm or deny it directly. Where a tradition is more diffuse, bundling rest, diet, social support, and symbolic ritual together, the research tends to land on real but modest benefit, driven more by the structured support than by any single restrictive rule.
The remission of symptoms was 2.57 times more likely in those taking Vitex agnus-castus extract than in those who received a placebo. (Meta-analysis of double-blind randomized controlled trials, Phytomedicine)
5. Menstrual Cycle Optimization: What Cycle Syncing Gets Right and Wrong
Cycle syncing, the practice of adjusting workouts, meals, and even work schedules to match the four phases of the menstrual cycle, has become a defining wellness trend of the mid-2020s. The underlying premise is reasonable on its face: estrogen and progesterone do fluctuate meaningfully across a cycle, and it would not be surprising if that affected performance or metabolism. The actual evidence is considerably less settled than the content built around it suggests.
What the sports science actually shows
A 2023 umbrella review in Frontiers in Sports and Active Living, led by exercise researcher Stuart Phillips’s group at McMaster University, examined the existing meta-analyses on menstrual cycle phase and resistance training and concluded that it is currently premature to claim that short-term hormonal fluctuations meaningfully affect strength performance or long-term training adaptations, citing highly inconsistent findings and widespread methodological weaknesses, such as inadequate verification of which cycle phase participants were actually in, across the underlying research.
A separate 2024 study from the Wu Tsai Human Performance Alliance, conducted with professional rugby league athletes, found that resting metabolic rate remained stable regardless of cycle phase or hormonal contraceptive use, suggesting female athletes do not need a different nutrition plan for each week of the month. That said, the science is actively evolving rather than settled in either direction: a large ongoing randomized trial, the IMPACT study, is directly testing whether periodizing training by cycle phase improves aerobic performance in well-trained women, and its results, once published, should meaningfully sharpen this picture.
What is worth keeping from the trend
None of this means menstrual cycle awareness is pointless. Many women do experience real symptoms, such as reduced tolerance for high-intensity training or changes in appetite, during specific phases, and tracking that pattern for oneself is reasonable and useful for planning. What current evidence does not support is the idea that every woman needs a categorically different diet or training program engineered around the four phases as a matter of physiology. The most defensible version of cycle awareness is personal symptom tracking, not a universal protocol sold as required science.
6. Hormonal Weight Gain: The Real Mechanism Behind a Popular Complaint
Weight gain around the menopause transition is one of the most consistent complaints in women’s health, and unlike some hormone-adjacent claims, it has a well-documented mechanism behind it. A comprehensive literature review in Climacteric found that while weight gain itself cannot be attributed to the menopause transition alone, since most of it tracks with normal aging in men too, the change in hormonal environment at menopause is clearly associated with an increase in total body fat and, specifically, a shift toward abdominal fat storage. Animal studies cited in the same review found that loss of ovarian hormone function promotes diet-independent increases in fat tissue and related metabolic changes.
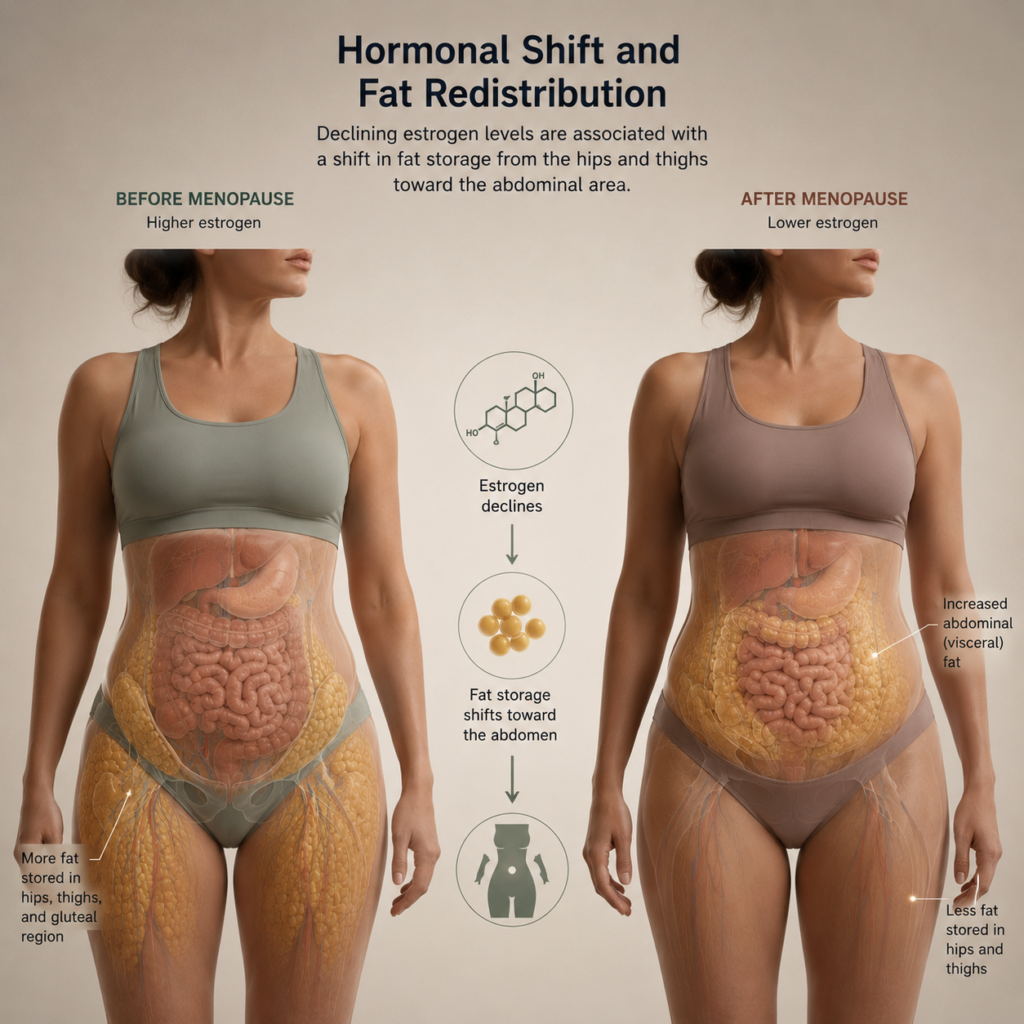
Insulin resistance compounds the picture. Declining estrogen reduces insulin sensitivity, and the resulting rise in circulating insulin favors fat storage, particularly viscerally, according to a clinical summary from Madison Women’s Clinic. This creates a self-reinforcing loop: abdominal fat is itself metabolically active tissue that further worsens insulin resistance. The Climacteric review notes there is strong evidence that estrogen therapy can partly prevent this specific pattern of fat redistribution, improving insulin sensitivity and reducing the rate of new type 2 diabetes, though as covered in Section 3, hormone therapy is not approved or recommended purely as a weight-loss intervention.
What actually helps
- Resistance training becomes more, not less, important during and after the menopause transition, both for preserving muscle mass that naturally declines with falling estrogen and for improving insulin sensitivity directly.
- Protein intake needs typically rise slightly to help counter age- and hormone-related muscle loss, alongside resistance training.
- Sleep quality has an outsized effect on insulin sensitivity and appetite-regulating hormones, and perimenopausal sleep disruption can independently worsen weight trends regardless of diet.
- A conversation with a clinician about hormone therapy timing, per the window of opportunity research in Section 3, is worth having specifically because of its documented effect on fat distribution and insulin sensitivity, separate from any effect on the scale.
7. Marketing vs. Medicine: Sorting Hormone Hype from Hormone Evidence
Few areas of wellness content borrow scientific vocabulary as freely as women’s hormonal health, and few areas have as wide a gap between what is said with confidence and what has actually been demonstrated. Two terms in particular are worth understanding clearly, because both sound clinical and neither is.
Estrogen dominance: a 1990s marketing term, not a diagnosis
Estrogen dominance describes a state where estrogen activity is disproportionately high relative to progesterone, and it is used constantly in wellness content to explain everything from PMS to weight gain to fibroids. The term was popularized in the 1990s by a physician advocating for natural progesterone therapy, and it is not recognized as a formal diagnosis by the American College of Obstetricians and Gynecologists, the American Academy of Family Physicians, or the Endocrine Society, according to a 2026 clinical review from the Menopause Consortium. There are no universally accepted lab thresholds that define it, and during perimenopause specifically, research shows estrogen fluctuates erratically rather than staying consistently elevated, which undercuts the simplified version of the theory sold in most wellness content, per a separate 2026 review from Winona. The underlying idea, that the ratio between estrogen and progesterone matters clinically, has some legitimate grounding in conditions like anovulation and luteal phase deficiency; the problem is the packaged diagnosis sold around it, complete with supplement protocols, rather than the physiology itself.
Seed cycling: marketed as ancient, invented far more recently
Seed cycling, eating specific seeds such as flax, pumpkin, sesame, and sunflower during different cycle phases to “balance” estrogen and progesterone, is frequently framed in marketing copy as an ancient or traditional practice. It is not. Unlike chasteberry, with its documented 2,500-year record, seed cycling is a naturopathic protocol that emerged in the late twentieth century with no comparable historical lineage. The evidence for it is genuinely preliminary: a 2025 systematic review in PMC covering ten small studies found seed cycling was associated with improved menstrual regularity and reduced PMS severity, but explicitly noted the conclusion rests on small sample sizes and low to moderate quality evidence, calling for larger randomized trials before firmer claims are warranted. A separate consumer-facing review from Healthline reaches a similar verdict: the plant compounds involved have only weak documented effects on hormone levels. Eating more flax and pumpkin seeds is a reasonable dietary choice on its own nutritional merits; treating it as a validated hormone-balancing protocol is not yet supported by the size or quality of the evidence.
A side-by-side comparison
Table 2. Popular hormone-related claims ranked by how strong the current evidence actually is.
| Claim or practice | Evidence status | What is actually known |
|---|---|---|
| Chasteberry (Vitex) for PMS | Strong | 2,500 years of use plus modern RCT meta-analysis (RR 2.57 vs placebo) |
| Lifestyle change / insulin sensitivity for PCOS | Strong | Recommended as first-line by international guidelines; direct mechanistic link |
| Early hormone therapy timing in perimenopause | Strong, emerging | New large-scale data supports a window of opportunity; still an active research area |
| Inositol for PCOS | Preliminary, mixed | Some metabolic benefit signal; guideline review calls evidence limited and inconclusive |
| Postpartum confinement (specific restrictions) | Weak for restrictions, moderate for support | Little evidence for specific taboos; benefit likely driven by rest and family support |
| Seed cycling | Preliminary | Small, low-to-moderate quality trials; not an ancient practice despite marketing framing |
| Adrenal fatigue / adrenal support supplements | Not supported | Systematic review of 58 studies found no evidence it exists as a condition |
| Estrogen dominance as a diagnosis | Not recognized | Not endorsed by ACOG, AAFP, or the Endocrine Society; no accepted lab threshold |
None of this is a reason to dismiss curiosity about hormonal health, quite the opposite. It is an argument for asking, before adopting a protocol, whether the claim behind it has actually been tested, and by whom.
Women’s hormonal health sits at an unusual intersection: genuinely complex, historically under-researched by mainstream medicine, and now heavily colonized by wellness marketing that borrows clinical language faster than clinical evidence can keep up. The honest picture that emerges from current research is less dramatic than most content promises, but more useful. Cortisol is not something to fear or detox, only something to manage through genuine stress reduction. PCOS is a metabolic condition worth taking seriously and getting properly diagnosed rather than guessed at. Perimenopause deserves an early, informed conversation with a clinician rather than a decade of silent symptom management. Cycle awareness is worth tracking personally without being sold as mandatory science. And a small number of old, specific remedies, chasteberry chief among them, have earned their reputation the hard way, through trials rather than tradition alone.
Sources & Further Reading
- Sterling Medical Center, How Your Stress Response Works: HPA Axis and Cortisol (2026)
- International Journal of Molecular Sciences, Chronic Stress and Autoimmunity: The Role of HPA Axis and Cortisol Dysregulation (2025)
- PMC, Adrenal fatigue does not exist: a systematic review
- TIME, Is Adrenal Fatigue Real? (2026)
- Cedars-Sinai, Is Adrenal Fatigue a Medical Myth?
- World Health Organization, Polycystic ovary syndrome fact sheet
- Journal of Clinical Endocrinology & Metabolism, Inositol for Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis (2023 guideline)
- Frontiers in Endocrinology, Effects of inositol in women with PCOS: an umbrella review (2026)
- The Menopause Society, When Women Initiate Estrogen Therapy Matters (2025)
- Epic Research, Hormone Replacement Therapy Prescriptions for Women Up 72% Since 2021
- American Family Physician, Menopause Management: When Hormone Therapy Is Appropriate (2026)
- American Academy of Family Physicians, Chasteberry clinical review
- Phytomedicine, Vitex agnus-castus in premenstrual syndrome: A meta-analysis of double-blind randomised controlled trials
- Grokipedia, Postpartum confinement: history and traditions
- PLOS One, Maternal postnatal confinement practices and postpartum depression in Chinese populations: A systematic review
- Frontiers in Sports and Active Living, Current evidence shows no influence of menstrual cycle phase on resistance training (2023)
- Wu Tsai Human Performance Alliance, Study challenges cycle syncing, finds metabolism consistent during menstrual cycle
- PMC, IMPACT study protocol: Menstrual cycle-based periodized training on aerobic performance
- Climacteric, Understanding weight gain at menopause
- Madison Women’s Clinic, Menopause and Insulin Resistance
- The Menopause Consortium, Oestrogen Dominance: A Popular Term, Not a Medical One (2026)
- Winona, The Myth of Estrogen Dominance (2026)
- PMC, Efficacy of Seed Cycling as an Integrative Therapy for PMS and PCOS: A Systematic Review (2025)
- Healthline, What Is Seed Cycling? Effects on Hormones and Menopause
This article is for general informational purposes and does not constitute medical advice. Speak with a qualified healthcare provider, such as a gynecologist or endocrinologist, before making significant changes to hormone therapy, supplementation, or diagnostic testing, particularly if you manage a chronic condition.

